
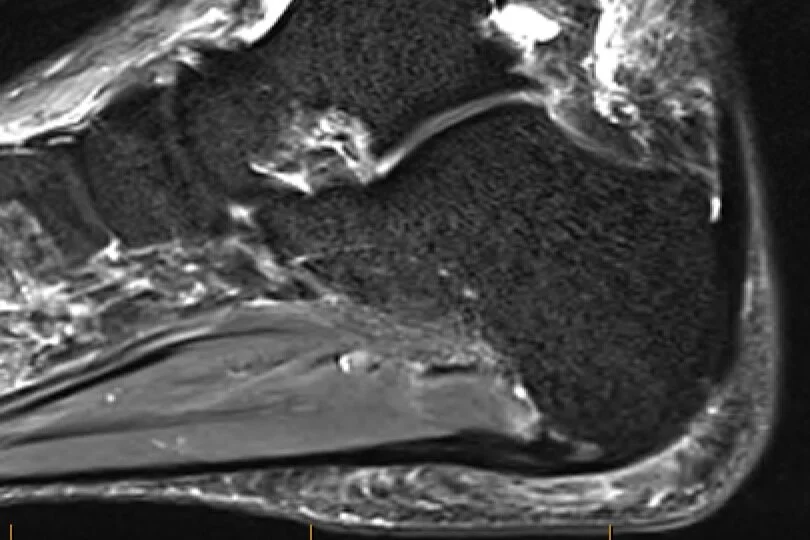
MRI scan showing changes in plantar fascia origin consistent with plantar fasciitis
Plantar fasciitis is localised inflammation and degeneration of the proximal plantar aponeurosis (plantar fascia) most commonly near the origin at the medial calcaneal tuberosity of the calcaneus (heal bone).
The strongest risk factor is obesity. There is evidence hamstring inflexibility (tightness) also plays a role. There is inconclusive evidence physical activity, including weight bearing endurance activity and prolonged standing; deceased ankle dorsiflexion (extension, upwards bend) due to calf tightness; reduced toe flexion (downwards bend) strength, and foot ‘posture’ are risk factors.
Heel spurs are not a risk factor for plantar fasciitis. They reside in the short muscles of the foot, not the plantar fascia; are common, present in 1 in 10 (10%) people; and only 1 in 20 people (20%) with heel spurs have heel pain.
Plantar fasciitis initially presents with sharp localised medial (inside) heel pain that has a ‘start-up’ quality that it is worse on arising from bed in the morning or when going from sitting to standing. Eventually it is replaced by an ache that is worse at the end of the day or after prolonged standing.
On examination there is usually tenderness over the medial calcaneal tuberosity (inside heel) and pain on dorsiflexion (bending up) of the ankle and toes. There is usually also calf tightness.
Other possible causes of similar heel pain that need to be ruled out include Baxter’s neuropathy (entrapment of the 1st branch of the lateral plantar nerve), tarsal tunnel syndrome, heel fat pad contusion, Achilles tendinopathy, tibias posterior dysfunction, calcaneal stress injury, subtalar joint arthritis, and inflammatory arthritis.
Most cases, 80-90%, resolve within 10 months. A small proportion of cases do not resolve without treatment.
Plain radiographs (XRays) are usually normal. Diagnostic ultrasound scanning may show thickening (> 4 mm thickness), hypoechogenecity (dark appearance), hyperaemia (increased blood flow), and intrasubstance tearing. MRI scanning can additionally show bone marrow oedema at the calcaneal enthesis (‘bone bruising’ in the heel bone) and perifascial oedema (swelling around the plantar fascia).
Treatment should include addressing the risk factors including weight loss, relative rest from painful activity, hamstring and calf stretching, and foot muscle (short foot and high load) strengthening. Plantar fascia specific stretching can also be beneficial as well as topical ice and non-steroidal anti-inflammatory medications (NSAIDs). Low-dye taping may provide short-term relief and can be helpful in determining if an orthotic is likely to be effective. Immobilisation in a cam-walking boot for 8-10 weeks can help settle acute disabling pain while a custom rather than prefabricated night-splint can improve day-to-day pain.

High Load Strengthening

Plantar Fascia Specific Stretching
Custom orthotics have not been shown to be more beneficial than simple soft off-the-shelf orthotics. A soft off-the-shelf orthotic incorporating a heel cut-out and plantar fascia groove, to support the medial longitudinal arch of the foot and reduce direct pressure on the the plantar fascia while also reducing tension in the plantar fascia, can be effective particularly if low-dye taping of the foot provides some pain relief.
The ultrasound guided perifascial (underneath and beneath the plantar fascia) injection of cortisone can provide patients with 6-8 weeks of relief. The costisone should not be injected into the plantar fascia itself as it can tear the plantar fascia and weaken it as the corstisone is catabolic (‘breaks’ tissues down).
Focussed extracorporeal shockwave therapy is reserved for low-grade plantar fasciitis with the absence of intra-substance tears on scanning while the ultrasound guided intra-substance (into plantar fascia tear) injection of leukocyte-rich platelet-rich plasma (LR-PRP, high concentration of white blood cells and very high concentration of platelets), which induces a healing response within the plantar fascia over 12+ weeks, is reserved for chronic high-grade plantar fasciitis with intra-substance tears on scanning and symptoms of greater than 6-12 months.

Focussed Extracorpreal Shockwave Therapy (Storz Duolith SD1 T-Top Shockwave Source)
Very rarely is surgery warranted.